The Chemicals of Love
Intimacy
Feelings of intimacy are primarily driven by and release the neurotransmitters Dopamine and Norepinephrine.
Dopamine is the primary reward chemical and responsible for a positive response to stimuli and the feeling that we should keep doing exactly what we're doing. When we abuse substances our ability to produce dopamine naturally is drastically reduced. Our brains adjust to the artificial dopamine flooding of drugs and alcohol by slowing and stopping natural production. So, we begin to experience extreme lows with no sense of reward in anything but substance use. Substance use itself also loses efficacy, so we have to use more, more often in order to just maintain. In early recovery, Dopamine levels remain low until our brains heal and re-balance themselves. When Dopamine is low, or missing, we lose the ability to feel feelings of intimacy. My personal theory is that that is why addicts so often start to isolate. We can't feel any reward in being with others any more.
Norepinephrine is an excitatory neurotransmitter and is responsible for increased energy, attention and focus. On the positive side it can create feelings of euphoria, while on the negative it can be activating and stressing enough to create anxiety and panic attacks. In terms of intimacy, Norepinephrine drives the butterflies in the stomach and inability to stop thinking about someone. Norepinephrine is decreased in the short term by depressants like alcohol, while it is dramatically increased by stimulants. With stimulants norepinephrine suffers the same fate as dopamine, we lose the ability to produce our own while using, and so experience extreme lows when not actively using.
Passion
Feelings of passion are driven by the primary sex hormones Testosterone and Estrogen, which are responsible for arousal and desire.
With Testosterone, in the short term, there is an acute increase in all sexes with consumption of alcohol and stimulants. Through a series of reactions the long term result is the same as with the neurotransmitters of intimacy, natural production slows and stops. In between using and when first getting sober, people suffer extreme lows and often have difficulties with arousal and desire. ED, low libido, and depression are common testosterone related effects of substance abuse. With opiates there is a short term decrease which can be followed by a sharp increase and what is sometimes called "rebound libido" when getting sober.
Estrogen is increased in the short term in all sexes with alcohol consumption too, though it is unclear whether there is an eventual backlash of reduced levels. Because of the increase, there is an increased risk of breast cancer in AFAB people and of erectile dysfunction in AMAB people. Estrogen is decreased in the short term with fentanyl, gabapentin and tramadol abuse which can cause vaginal dryness, painful sex and lack of desire.
Commitment
Feelings of commitment are driven by Oxytocin and Vasopressin, which are the hormones responsible for pack and pair bonding. Both are present in all sexes, but generally speaking, Oxytocin is primary in AFAB people, and Vasopressin (a primitive form of oxytocin) is primary in AMAB people. These two hormones are very similar in function, except Vasopressin's form of familial and romantic bonding tends to be more about protection and defense.
In the short term, Oxytocin levels decrease with alcohol and opiate consumption, which can create difficulties in familial and romantic bonding. Interestingly, Testosterone is an Oxytocin blocker, so Oxytocin levels decrease with higher testosterone levels and increase with lower testosterone levels.
Like Oxytocin, Vasopressin decreases with alcohol and opiate consumption, creating similar difficulties in relation to others.
Stay tuned for more about what love is and is not.
Styles of Love
According to Robert Stenberg's triangular theory of love, there are several styles of love, or ways of loving, that come from various combinations of the three parts.
If there is intimacy alone, he calls that a "liking love." Essentially the love of close friends.
If there is commitment alone, he calls that "empty love." There might be a better name for it, but it is referred to this way out of the assumption that the other two parts were present, but lost somewhere along the way.
Passion alone is called "infatuation." Some might call it lust as well.
When intimacy and passion are present without commitment, he calls that "romantic love." This is the kind of love we see in most media, the kind that takes you all the way up to the altar, but not through the next 20 years of the ups and downs of day to day life.
When passion and commitment are present without intimacy, it is called "fatuous love," which means foolish or foolhardy love. It's the kind of love Elvis talks about in the song "Fools Rush In."
When commitment and intimacy are present, Stenberg calls it "companionate love." The love of close companions.
When all three are present, he calls it "consummate love," which means a perfect or complete love. This operates under the assumption that everyone wants some balance of all three elements, which is not necessarily true.
Any individual element or combination is a valid kind of love if that's what someone wants and they are engaging that way with intention. Where we go sideways is when we are engaging in love styles that don't suit us, or that we don't actually want. We may have difficulty with one element or another and so settle for less.
Stay tuned for more about the neurotransmitters and hormones of love and how love is affected by drugs and alcohol.

What is Love?
One way to think about love is to use Robert Stenberg's Triangular Theory of Love. It is a model that says there are three primary parts to love; intimacy, passion, and commitment. According to this theory, a kind of love exists in each part on its own, and in any combination of the three parts. Each part is love. Any of the parts together is love. All three parts together are love.
Intimacy
According to Robert Stenberg's triangular theory of love, Intimacy is the "I know you" of love. Instead of being a euphemism for ***, intimacy means bonding, closeness, connection and open honesty between people. Intimacy occurs when someone has enough access to their vulnerability to let someone really know who they are. This is part of why people use and drink to feel connected, because it is difficult to be vulnerable in that way when you don't know how. In his triangular model, Stenberg calls love that consists of only intimacy, without passion or commitment, "liking love."
Passion
Stenberg says that passion is the "I want you" of love. Passion means excitement, attraction, desire, and arousal. It is the heat of love. Passion occurs when someone has enough access to their vulnerability to feel how they feel and want what they want. This is part of why people use and drink to feel impassioned, because it is difficult to be vulnerable in that way when you don't know how. In his triangular model, Stenberg calls love that consists of only passion, without intimacy or commitment, "infatuation."
Commitment
According to Stenberg, commitment is the "I need you" of love. Any of the parts of love can be enacted in healthy or unhealthy ways and Commitment is no different. The unhealthy version would be something like codependence or enmeshment. Healthy commitment means interdependence, which is the ability to balance needing someone and being independent at the same time. It also means shared work/tasks/goals, day to day life, and the quality of enduring or getting through difficulties together. Commitment occurs when someone has enough access to their vulnerability to let themselves rely on another person. This is part of why people use and drink to manage feelings around commitments and to help have or avoid them, because it is difficult to be vulnerable in that way when you don't know how. In his triangular model, Stenberg calls love that consists of only commitment, without passion or intimacy, "empty love." I don't necessarily agree that commitment alone has to feel empty. People might choose this way of loving intentionally. Stenberg's background, however, is in couples therapy, so his perspective is of people who had the other two parts of love and lost them.
Stay tuned for more about the way these three parts of love interact.
Maslow’s Hierarchy of (Recovery) Needs
Maslow's Hierarchy of (Recovery) Needs
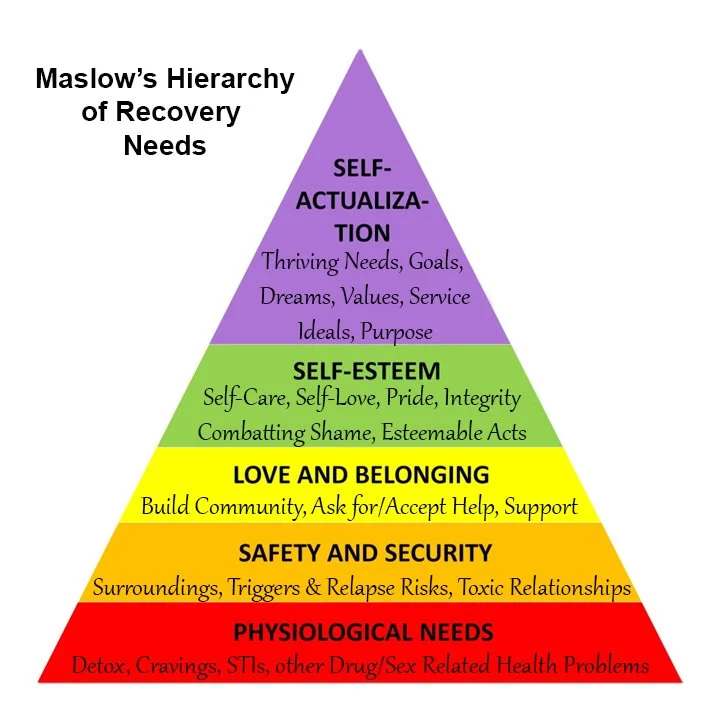
Maslow's Hierarchy of (Recovery) Needs! At the base of Maslow's pyramid are physiological needs which in this context are things like; detox/withdrawal symptoms, cravings, sex and drug related health issues, and STIs. The next part represents Safety and Security needs, which in this case are things like; safe surroundings, avoiding relapse risks and triggers, and exiting toxic relationships. The next section represents our Love and Belonging needs; building community, being able to ask for and accept help, and having a support system. The next part is our Self-Esteem needs which are things like; self-care, self-love, integrity, pride, combatting shame, and doing esteemable acts. Maslow's final section represents our Self-Actualization needs. These are things like; thriving needs, goals, dreams, values, ideals, being of service, and having purpose.
When you're thinking about using Maslow's Hierarchy of Needs, you start at the bottom and work your way up. If our lower level needs aren't met, we won't be able to focus or make progress on meeting a higher level of needs. For example: if we're in active detox, we won't be able to focus on making our surroundings safe. If our surroundings aren't safe, we won't be able to work on building a support system. Without any support, we won't be able to make progress on building self esteem through esteemable acts. If we have no self-esteem, we won't be able to focus on our thriving needs. Each lower level need we meet, then allows us to make progress on the next level up.
It's also worth noting that the hierarchy isn't stagnant, so we may make a bunch of progress and move our way up, only to find that a new or reoccurring lower level need arises that has to be met before we can continue making good higher level progress.
This hierarchy isn't the only way to envision needs, but it can be very helpful in early recovery to help decide where to put your attention. Without it, we may experience things like having heavy cravings while struggling to work on our ideals. If we focus on managing physiological needs first, we will have an easier time getting those self-actualization needs met later on.
Even with a tool like this, sometimes it can be hard to cut through all the physical, mental, and emotional static and see clearly what your unmet needs are. If we can't separate one need from another how can we use Maslow's Hierarchy? Try starting with physiological needs and looking for pain, discomfort and dysregulation. If your physiological needs are stabilized, look for life stress, insecurity and general instability. If your Safety & Security needs are being met, look for loneliness and isolation. If your Love & Belonging needs are satisfied, look for negative self-talk and feeling the need to keep secrets or edit yourself. If your self-esteem needs are met look for feeling lost, purposeless, and feeling like your just surviving or going through the motions. If all of your needs are being met, keep actualizing. (And try to add some joy, fun, and pleasure in there.)
If you would like a printable worksheet of the Maslow’s Hierarchy of (Recovery) Needs questions, email RecoverAfterDark@gmail.com with the subject line “Maslow.”
Could I Be a Chemsex Addict?
Could I be Chemsex Addict?
If you are wondering whether or not you might be a Chemsex Addict, here are some questions to ask yourself. The first is whether or not you have used meth or cocaine, possibly in combination with other drugs, to intensify sex or to have the kind of sex you want to have. If not, you can stop right here, because you haven’t engaged in Chemsex. If your answer is yes, you have engaged in Chemsex to some degree, so you should continue on to the next four questions.
1. Have you engaged in Chemsex on a regular basis, all the time, or to what feels like excess?
2. Are you showing signs of addiction like; tolerance, loss of control, unsuccessful at moderating or stopping, continuing despite consequences, excess time spent preparing or recovering, and/or withdrawal?
3. Have you relapsed or do you feel like you might relapse in order to have sex?
4. Have you had, or do you want to have, sex with a strong or guaranteed risk for relapse?
If you answered yes to any of the last four questions, you may be a Chemsex Addict. At the very least, sex is likely going to be an issue that needs to be addressed right away in recovery. If you answered yes to multiple questions, you will run an extremely high risk of relapse if you don’t address sex immediately in recovery.
If you would like a printable worksheet for these questions, email me at recoverafterdark@gmail.com with the subject line Chemsex.
What is Chemsex Addiction?
What is Chemsex Addiction?
Chemsex addiction occurs when a person switches from enjoying casual or even intense substance use in combination with sex to experiencing the effects of addiction. The rewards begin to be outweighed by the consequences. Harm reduction methods can still help and keep a person alive, but they become less effective and maybe just not enough. A person may feel completely dependent on chems to have sex at all. Sex outside of the drug experience may seem lackluster or even unpleasant. The classic signs of addiction like developing tolerance and inability to stop or moderate start to show up strongly. A person may feel like their sexual behavior is out of control. A lot of Chemsex addicts are mistakenly “diagnosed” as “Sex Addicts.”
And that is the primary difficulty for Chemsex addicts, a perfectly normal and nearly automatic human function becomes entangled with something that almost always requires complete abstinence to fully recover. Folks are often trying to moderate one thing and stop the other, while not getting any help with detangling the two. In fact, it is often recommended to put sex on the back burner, or just “wait a year,” but with no guidance about when to approach the back burner, or what to do while you’re waiting.
I’ve seen so many people relapse over sex. They can stay sober while they’re abstinent from everything, but as soon as sex comes back into the picture, all the old habits and mental/emotional/physical entanglements are still there. Sex will only stay on the back burner for so long before it becomes a problem. I like to say that the back burner is where things catch on fire.
This is why we have to bring everything up front and address it right away.
What is Chemsex?
What is Chemsex, Party n Play, PnP?
Chemsex, also known as Party n Play or PnP, is a term that comes from the London gay club scene of the 90’s. At the time it was a term specific to gay men, and referred to using stimulants (usually meth) with other euphoria inducing drugs (usually ghb) in combination with sex in a party setting. As the practice became a cultural movement, it shifted from the clubs to bathhouses, adult bookstores, and other more private scenes where sex and drug use could be the main focus.
Now, Chemsex is deeply imbedded in queer culture and has grown to include the whole spectrum of LGBTQ+ folks as well as straight identified men who have sex with men. Other substances like ketamine and ecstasy are often involved, but meth is usually still the primary drug of choice. The biggest change has been hookup apps becoming the primary method of people finding sex partners and drug connections, as opposed to cruising and circuit parties.
Other folks, not LGBTQ+ identified, also use substances, including meth, in casual sex and party situations, but a big part of Chemsex is in the specificity of the culture and how it both benefits and harms LGBTQ+ communities.
Will My Enabling Use Be a Problem in Recovery?
Will my enabling use be a problem in recovery?
If you’re wondering if your enabling use might be an issue in your recovery that needs to be directly addressed, here are some questions to ask yourself. The first is whether or not you have used in the past to make sex possible, easier to have, or more pleasurable. If not, you can stop here because you have not engaged in “Enabling Use” as we’re defining it here. If your answer is yes, you have engaged in enabling use to some degree, so you should continue to the next four questions.
1. Have you used substances to make sex possible or better on a regular basis or all the time?
2. Have you rarely or never had sex sober?
3. Do you have a hard time imagining a sex life without substances?
4. Have you relapsed or do you feel like you might relapse in order to have sex or because you had sex?
If you answered yes to any of the last four questions, sex is fairly likely to come up as a relapse risk in recovery and should be addressed sooner rather than later. If you answered yes to multiple questions, sex is almost guaranteed to be problematic if it goes unaddressed for too long in your recovery.
If you would like a printable worksheet for these questions, email me at recoverafterdark@gmail.com with the subject line Enabling Use.

What is Enabling Use?
What is enabling use?
“Enabling Use” is a term I use to describe the entire spectrum of using substances to make sex more intense, more pleasurable, or even possible in the first place. This spectrum ranges from infrequent/low intensity to very frequent/high intensity. On one end of the spectrum, a person might have a drink to deal with the first date jitters. On the other end of the spectrum, a person might be completely dependent on substances to make sex happen or maybe they’ve never had sober sex at all.
This is an important thing to consider in early recovery because the more closely intertwined these things are, the more difficult it can be to stay sober. The more closely intertwined these things are, the more necessary it will be to address sex and substance use at the same time.